 Application Form for Qualification
Application Form for Qualification








1. Application_Form_for_Qualification.hwp
2. Application_Form_for_Qualification.doc
Application_Form_for_Qualification.doc
3. Application_Form_for_Qualification.pdf
Application_Form_for_Qualification.pdf
2.
3.
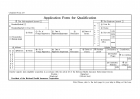


Application Form for Qualification

Application Form for Qualification
The Self-employed Insured □
The Employee Insured □
①
Household(whole) □
WorkplaceCorporatIon
② Code No.
Household(partial) □ (Card No: )
③ Name
□ Householder
□ Employee Insured
⑥ Name
⑦ No. of
Foreign Registration
⑧ Date of
Registration/Employment
⑨ Nationality
⑩ Status of Sojourn
④ Unit site
code
name
⑤ Business
office
code
name
⑪ Address
Cellular Phone( )
□□
ID
NE
SP
UE
RN
ED
DA
NT
⑫Relation
⑬ Name
⑭ No. of
Foreign Registration
⑮ Date of
Registration /Employment
Nationality
Status of Sojourn
Resident
period
Declaration of Contribution, etc.
Monthly
Wages
Accounting
code
Contribution Reduction
Job Category
code
code
I hereby register alien eligibility acquisition in accordance with the article 45 of the National Health Insurance Enforcement Decree.
Enrollee : (Signature)
(Employer) (Official Seal)
President of the National Health Insurance Corporation
Note) Please, refer to the back page for your help in filling out the form.

-
Application Form for Tax Reduction or Exemption,Application Form in regards to a Change in the Content of Tax Reduction or Exemption
[Form No. 80] (01.3.28. 개정) Foreign Investment □Application Form for Tax Reduction or Exemption □Application Form in regards to a Change in the Content of Tax Reduction or Exemption Term of .. -
Application Form for Prior Checking of Tax Reduction or Exemption
[Form No. 81] (00.3.30.개정) Foreign Investment Application Form for Prior Checking of Tax Reduction or Exemption Term of Processing 20 Days Applicant ①Name ②Nationality ③Address (Tel.. -
Application Form for Prior Checking of Tax Reduction or Exemption
[Form No. 81] (00.3.30.개정) Foreign Investment Application Form for Prior Checking of Tax Reduction or Exemption Term of Processing 20 Days Applicant ①Name ②Nationality ③Address (Tel.. -
Application for Tax-Exemption on Non-Resident's Korean Source Income Provided under the Korea Tax Treaty(Corporate Income tax,Individual Income tax)
Form 29-2 (1) □ Interest □ Dividends □ Royalties □ Other Application for Tax-Exemption on Non-Resident's Korean Source Income Provided under the Korea Tax Treaty □ Corporate Income tax □ Individual.. -
FoodExpoApplicationForm
Food Expo Application Form 1. Description of Application Description Contents Company Name President Address Postal Code( ) Person in Charge Name : Title : Tel Fax E-mail H.. -
영문 이력서(IT관련업체)
C.Dayamayi Career Summary: Around 2.1 years of IT experience in development, Training and testing of application software using C, C++, VC++(5.0/6.0) MFC/ATL, COM/DCOM, Oracle and design tools.. -
E.E.C ENGLISH PROGRAM IN KOREA
E.E.C ENGLISH PROGRAM IN KOREA Application Form Please follow the application form instruction 1. Name : Last Attach a passport size photo taken within last six months First Middl.. -
해외자원봉사 지원서 작성 샘플(국제기독청년교류 ICYE)
Application Form(해외자원봉사지원양식)을 실제적으로 작성한 사례입니다. 부족한 점이 많지만 이런 양식을 참고하시면 좋을 듯 싶습니다. ^^ <본문내용> ■ I am interested in being a Volunteer! What Country.. -
영문 신청서
APPLICATION FORM 1. Personal Information 2. Application Field (list area you apply to) 3. Edu cation (list education and training details in reversechronological order) 4. English Profi.. -
영문 신청서
APPLICATION FORM 1. Personal Information 2. Application Field (list area you apply to) 3. Edu cation (list education and training details in reversechronological order) 4. English Profi..

